Unburdened by false humility, postmodern trauma activists claim to have understood for the first time what drives all of human suffering
Trauma DispatchTrauma news you can't get anywhere else. |
|
|
CATEGORY: GOVERNMENT PROJECTS  Jim Kenney (D), former mayor of Philadelphia; Danielle Outlaw, former Police Commissioner Source: City Journal Read time: 1.7 minutes This Happened Trying to reverse Philadelphia’s slide as one of the worst major cities in the United States for homicides, violence, and crime, new mayor Cherelle Parker (D) declared a state of emergency based on crime In January 2024 immediately after taking office. During the 2023 race for mayor, Parker ran as a moderate compared to other progressive candidates by prioritizing public safety. She also selected new police commissioner Kevin Bethel. Since coming into office Mayor Parker and Commissioner Bethel cleared out the infamous Kensington open-air drug market and cracked down on illegal packs of ATV and dirt-bike riders. Why Is This Happening? These changes came on the heels of previous mayor Jim Kenney (D) who had refused to declare a state of emergency despite record homicides. The city had 561 murders in 2021, its highest total ever; 80% of victims were Black. Kenney had supported defunding the police and sanctuary city status. Bethel’s predecessor as police commissioner was Danielle Outlaw, who was lured from Portland, Oregon and hired in 2020. Emphasizing her status as the first Black woman to lead the police departments in Portland and Philadelphia, she had promised to tackle racism, gender discrimination, social injustice, inequity, and most of all, gun violence. Outlaw resigned in September 2023, shortly before the mayoral election, after three years of worsening crime under her watch. Philadelphia’s crime problems are also worsened by the policies of progressive DA Larry Krasner, who remains in office. The background of crime in Philadelphia, however, has older roots in the city’s failed attempts to use trauma-informed approaches. The Trauma-Informed Past of Philadelphia Philadelphia was the first major city to deploy large-scale public health efforts under the banner of trauma and toxic stress. As described in my book, The Trouble With Trauma: “In 2005, the Philadelphia Department of Behavioral Health and Intellectual Disability Services initiated a transformation of the city’s mental health services in order to address high unemployment and murder rates. The keystone of this transformation was the creation of a trauma-informed system based on the premise that exposure to trauma and violence was causing these problems with unemployment and murder. The transformation included efforts to train clinicians in evidence-based psychotherapy for PTSD, and to bring together a large number of community human-service organizations to train their staff according to the Adverse Childhood Experiences studies.” [1] Pulling together mental health experts, politicians, public health, and law enforcement, the plan essentially cast trauma as the largest public health issue we face in modern times, and we need massive funding for social programs to attack trauma on the order of the Manhattan Project that created the first nuclear bomb. It was supposed to address racism, inequities, and reduce violent crime. Mayor Parker’s new crackdown on crime and sudden rediscovery of law and order seems to confirm that toxic stress public health efforts didn’t work. Neither the Mayor nor the police chief mentioned the failure of the 2005 trauma-informed initiatives. REFERENCES [1] Scheeringa MS (2022). The Trouble With Trauma: The Search to Discover How Beliefs Become Facts. Las Vegas: Central Recovery Press. ISBN 978-1949481563 Like Trauma Dispatch? You can subscribe to our email notices of new posts on this page. CATEGORY: GOVERNMENT PROJECTS  Megan Carson, First 5 Mendocino Commission Source: National Association of Counties Read time: 1.9 minutes This Happened First 5 Mendocino Commission brought together 42 agencies that support children’s wellbeing for its annual State of the Child summit in March. Speakers stressed that it is possible for children who encountered adverse childhood experiences (ACEs) to grow beyond those experiences. Who Did This? First 5 Mendocino is a government agency that falls under the California Children and Families Commission, also known as First 5 California. It is one of 58 county commissions funded by a California state proposition tax. The board that runs First 5 Mendocino is appointed by elected officials. Their charge is to create, support, or promote programs in the community focused on healthy child development in the first five years of life. The operationalization of that mission is an overarching metric of equity [1]. They emphasize that oppression, including institutional racism, creates intergenerational trauma. First 5 embraces the ACEs and toxic stress narratives which claim that “the events of childhood shape a person’s biology, personality, dreams, and aspirations: their entire trajectory of life” [1]. Their stance is that “very few families have the support they need” and it is the government’s job to provide them (pages 12-14). The Premise The premise of the summit was to shift participants’ focus to resilience. For the past two decades, the trauma advocacy movement was fixated on promoting the theory of brain damage caused by trauma. Megan Carson, Community Outreach Leader, said, “What we also started to realize was that people were getting hung up on that and losing hope.” The adjacent graphic shows the tree analogy, a fixture of the ACEs and toxic stress narratives, which displays an extraordinary assortment of societal stressors that presumably damage children’s brains and physical health [1].  Speakers included Tina Payne Bryson, social worker, director of a play therapy institute and book author who claims her works deploys the latest neurobiology research on the power of relationships to shape brain architecture and mold personalities. Georgie Wisen-Vincent, marriage and family counselor, co-author with Bryson, and director of the play therapy institute, advocates using play to process traumas. MaryCatherine McDonald, PhD, has been skeptical of using ACE scores to predict individual outcomes, and wrote a book that reframes trauma responses as the body’s natural adaptive responses rather than the breakage of fragile humans. Analysis Many within the sprawling movements of ACEs, toxic stress, and trauma-informed approaches have realized that they have a bit of a messaging problem. While their message that trauma damages the brain has been an eye-popping success at gaining adherents, the acceptance of this belief system ultimately can be a downer. It is ironic that movements that were born from marketing rhetoric find themselves hamstrung by their message. As a result, there has been a slew of branding by many groups to highlight resilience. Agencies [2], projects [3], bills [4], and a documentary [5] have incorporated resilience into their titles. Oprah Winfrey and her frequent guest, child psychologist Bruce Perry, have staked one of the most extreme positions that a nurturing relationship in the first two months of life represents a nearly irreversible period for neural development [6]. The science of resilience, however, is as misguided as the science of the trauma narrative that it supersedes. Both are based on the claim that humans are highly malleable and life experiences can mold nearly every aspect of character and predict human flourishing. While the virtue of providing good care for young children is not disputed, the claim that parenting practices can shape the architecture of brains and impact adult physical illnesses is unproven and disputed by empirical research [7]. REFERENCES [1] 2021-2026 Strategic Plan. First 5 Mendocino Commission. https://first5mendocino.org/first5-flipbook/PDF.pdf [2] Doña Ana County Resilience Leaders (New Mexico); UCLA-UCSF ACEs Aware Family Resilience Network; Hawaii Governor’s Office of Wellness and Resilience; Idaho Resilience Project [3] Healthier Together Initiative Growing Resilience in Teens (GRIT) Grant Program (Philadelphia); North Carolina Center for Resilience & Learning; Community Resilience Initiative (Washington state); MassBay Community College, Institute for Trauma, Adversity, and Resilience in Higher Education [4] Resilience, Investment, Support, and Expansion from Trauma Act, federal H.R. 4541 bill [5] Resilience: The Biology of Stress & the Science of Hope (2016). James Redford and Karen Pritzker (producers). KJPR Films. [6] Bruce D. Perry, M.D., Ph.D. & Oprah Winfrey (2021) What Happened To You? Conversations On Trauma, Resilience, and Healing. New York: Flatiron Books [7] Judith Rich Harris (1998), The Nurture Assumption: Why Children Turn Out the Way They Do. New York: Free Press Scheeringa MS (2018). They’ll Never Be The Same: A Parent’s Guide to PTSD in Youth. Las Vegas: Central Recovery Press. ISBN 978-1942094616 Like Trauma Dispatch? You can subscribe to our email notices of new posts on this page. CATEGORY: GOVERNMENT PROJECTS  Nancy Osborn, MEd, PhD, KC Healthy Kids Source: KSHB 41 Kansas City Read time: 1.4 minutes plus 30-second video This Happened In June, 2024, a local nonprofit called KC Healthy Kids provided trauma-informed training for librarians and staff of Kansas City public libraries. Who Did This? The training was provided by counseling psychologist Nancy Osborn, MEd, PhD with KC Healthy Kids. Funding for the training was provided by the city of Kansas City, Missouri. The Premise The need for the training was described as library patrons often bring the problems of the outside world with them, such as not being civil, mental illness, and homeless people. According to the KC Healthy Kids website, their training includes the standard topics of trauma-informed care:
The 30-second video below explains what the training might accomplish: Another aspect that is common to all trauma-informed trainings is the claim that the science has been settled that trauma embeds itself in your body, damages brain centers, and rewires neural networks. The assertion of this neuroscience narrative is taken as settled science in trainings and serves as the crisis that makes these trainings so urgent. Analysis Despite the assertion of trainers, the science does not show conclusively that trauma damages brains. As Trauma Dispatch has documented here and here, the toxic stress and adverse childhood experiences narratives are based on weak, cross-sectional studies. When pre-trauma, prospective studies have been conducted, they consistently do not support the stress-damages-the-brain theory [1]. Rather than trauma causing brain changes, a more likely theory, and biologically much more plausible, is that of preexisting differences (also known as diathesis stress theory)—individuals who are vulnerable to the psychological effects of trauma had brain differences based on genetics that existed prior to experiencing trauma. Does it really help to approach difficult patrons from the stance that they could be trauma victims? Here, understanding their claims of brain damage is a crucial point. Activists would like us to believe that their approach is based on science. But realizing the evidence is absent, it’s clear that trauma-informed care is an ideology, making it evident that the point is not about actually helping patrons. It’s about installing an intellectual framework in society that humans are fragile, one training at a time. This framework of human nature has been underlying progressive leftist theory since Marx’s moral prophecies were promoted as science, and can be traced even earlier in philosophies such as Rousseau’s noble savage. As the reporter said in the video: the most important goal of training is to create a perspective shift. REFERENCES [1] Andrea Danese et al. "The origins of cognitive deficits in victimized children: Implications for neuroscientists and clinicians," American Journal of Psychiatry 174 (2017): 349-361. Julia A. DiGangi et al. “Pretrauma risk factors for posttraumatic stress disorder: A systematic review of the literature.” Clinical Psychology Review 33 (2013):728-744. Michael S. Scheeringa. "Reexamination of diathesis stress and neurotoxic stress theories: A qualitative review of pre-trauma neurobiology in relation to posttraumatic stress symptoms," International Journal of Methods in Psychiatric Research (2020). Like Trauma Dispatch? You can subscribe to our email notices of new posts on this page. CATEGORY: GOVERNMENT PROJECTS  Mikey Latner, founder, Project:Camp Source: WESH 2 news Read time: 2.5 minutes This Happened The staff of a traveling camp to help children cope with disaster held a practice camp with local agencies in Seminole County, Florida to prepare for the next hurricane. Who Did This? Project:Camp bills itself as a disaster response organization, traveling nationwide to provide free, trauma-informed childcare for families impacted by natural disasters. Based in Los Angeles, their team travels the country to set up pop-up camps, often in collaboration with a local government agency. Their website touts experience with a fire in New Mexico, tornados in Iowa and Oklahoma, and the Maui wildfire. Mikey Latner, a former camp director, is the founder of Project:Camp. The Premise At the practice camp, children engaged in typical camp activities, such as science and art projects, and watched movies. In addition, they were encouraged to process their feelings in gratitude circles and regular check-ins. This pilot camp was a collaboration with the Seminole County Emergency Management office. The camps seem to have two purposes. One is to provide childcare; give children safe, fun activities while parents can focus on disaster recovery. The other is therapeutic; to help children deal with their negative feelings about the disaster. The Project:Camp website asserts that the camps use a trauma-informed model to “help break up the formation of trauma.” It’s not clear what formation of trauma means, but it likely means to reduce post-traumatic stress symptoms. Analysis The childcare aspect of the camps appear to be an imaginative method that helps parents focus their time and energy on disaster cleanup and repair. But there are many concerns about the therapeutic activities that the camp organizers do not seem aware of. First, there doesn’t seem to be a requirement that children have emotional issues following disasters to attend the camps. It’s not clear that any children who enroll will need emotional assistance. Second, as recent surveys have shown major increases in youths acknowledging their unhappines, arguments have been made that this may be an unintended consequence of society and overconcerned adults constantly sending messages to children that they are fragile [1]. It is possible that gratitude circles and emotional check-ins will send messages to children that they should be upset about something, which may become a self-fulfilling prophecy. Third, their staff have much experience in running camps for children but do not include any licensed counselors or child development experts. Their board of directors and board of advisors also lack clinical experience. Fourth, the developmental expectations for these children seem unrealistic. Pre-adolescent children do not have fully-developed abstraction and self-reflection skills to understand when and why they should seek emotional assistance from adults and peers. Except perhaps for the more extroverted children, children have good intuition to not disclose scary feelings to virtual strangers. Fifth, universal interventions for individuals who are not asking for help have been shown to do more harm than good. Studies have shown that debriefing with adults immediately following traumatic events seems to worsen their symptoms [2]. Following 9/11 and Hurricane Katrina, agencies implemented universal interventions in classrooms; there was anecdotal evidence that showing images and recounting stories of the disaster were the first exposures some children experienced. Vicarious trauma was experienced by children in schools who had previously been protected from exposure to the disaster. Sixth, even if the camps could be helpful, it is unlikely that families will bring their children. Massive trauma treatment programs have already been attempted following 9/11, Hurricane Katrina, and the Queensland floods and they have all failed to attract many participants, even when services were free [3]. Seventh, while camp is a fun setting that may attract more individuals than prior post-disaster programs, there is no research support for this new method. Based on the large amount of experiences with disaster programs outlined above, this type of program that aims to help children is likely to provide no real help at all, and may instead cause harm. Why Is This Happening? Promoting itself as “trauma-informed childcare” [4] the camp is another iteration of the trauma-informed approach movement that has swept over the United States and other countries in the past ten years. Trauma has become the catchword of the decade [5] and the loadstar for all progressive policies to fix society’s ills. Trauma Dispatch has documented many of these programs in schools, courts, and government policies. REFERENCES [1] Shrier; Candice L. Odgers (May 21, 2024). The panic over smartphones doesn’t help teens. It may only make things worse. The Atlantic, https://www.theatlantic.com/technology/archive/2024/05/candice-odgers-teens-smartphones/678433/ Abigail Shrier (2024). Bad Therapy: Why the Kids Aren’t Growing Up. Sentinel. [2] Rose SC, Bisson J, Churchill R, Wessely S. Psychological debriefing for preventing posttraumatic stress disorder (PTSD). Cochrane Database of Systematic Reviews 2002, Issue 2. Art. No.: CD000560. DOI: 10.1002/14651858.CD000560. Accessed 23 June 2024. [3] Scheeringa MS, Cobham VE, McDermott B (2014). Policy and administrative issues for large-scale clinical interventions following disasters. Journal of Child and Adolescent Psychopharmacology 24(1), 39-46, doi: 10.1089/cap.2013.0067. [4] Project:Camp website, https://projectcamp.co/preparing-communities [5] Lexi Pandell (January 25, 2022). How trauma became the word of the decade. Vox, https://www.vox.com/the-highlight/22876522/trauma-covid-word-origin-mental-health Like Trauma Dispatch? You can subscribe to our email notices of new posts on this page. CATEGORY: GOVERNMENT PROJECTS  Victoria Woodards, Mayor of Tacoma, WA Source: Newsweek Read time: 1.5 minutes This Happened In Tacoma, Washington, 175 residents will be given $500 per month for twelve months to spend any way they want to help combat toxic stress. The program, called GRIT 2.0, started cash disbursements in April 2024. Who Is Doing This? The program is the brainchild of Victoria Woodards, the mayor of Tacoma since 2018. She sees her role as mayor is to embed equity into every policy to transform the city into being anti-racist. She makes decisions based on the Tacoma Equity Index, which rates neighborhoods on 32 indicators. For example, instead of fixing street lights based on who called to complain, she fixes street lights in neighborhoods where more equity is needed. Her administration has an Office of Equity and Human Rights that she helped establish, a Chief Equity Officer, and each city department must have a Racial Equity Action Plan [1]. Woodards was one of eleven mayors who founded Mayors For A Guaranteed Income in 2020 [2]. Despite her efforts, the city has struggled with a doubling of violent crime [3] and attracts large numbers of homeless people. The Premise Cash payments come from the Growing Resilience in Tacoma (GRIT) program. It was created in 2020 by Mayor Woodards as a way to demonstrate that cash to low-income families can reduce “toxic stress, improve economic stability, increase housing security, and improve health and well-being” [4]. In 2021-2022, GRIT 1.0 gave $500 per month to 110 participants for 13 months for a total of $715,000. Funding came mostly from a grant from Mayors for a Guaranteed Income [5]. GRIT 2.0 is a slight expansion of the program to 175 families. Analysis Prior to launching GRIT 2.0, there was no outcome evaluation of GRIT 1.0 to determine if any of the outcomes related to toxic stress were achieved such as improved economic stability, housing security, mental health, or reduced poverty. Supporters of cash assistance programs claim that support for a guaranteed income is as old as the United States [6]. Supporters fail to mention that much of that support has been suggestions to reform an unfair and wasteful welfare program, and often included incentives to work, as opposed to GRIT, which is an unconditional cash transfer. Cash transfers have been criticized as creating resentment, disincentivizing people to work, and morally wrong. National support has failed to materialize for these programs due in part to long-standing criticisms that they take money from people who work hard and give it to those who refuse to work or who purposefully have children out of wedlock. A 2017 review of 34 programs optimistically concluded that the effectiveness of cash transfers “remains very uncertain,” while failing to find any robust effects [7]. Trauma Dispatch has documented the lack of evidence for the toxic stress narrative here. Why Is This Happening? Dozens of small programs across the United States have been created for giving no-strings-attached funds to low-income individuals. All of these happened in areas run by progressive leftist politicians whose ideology is consistent with Marxist theory that problems of individuals are created by oppressors in society, and Communist- and socialist-style government solutions are needed to redistribute wealth. The Mayors for a Guaranteed Income coalition plans to use these programs to advocate for a federally-supported guaranteed income [8] This is an example of how the false narrative of toxic stress is leveraged by radical leftists. Victoria Woodards appears to have visions of utopian societies and justifies her policy decisions by claiming they are based on the science of toxic stress. REFERENCES [1] Podcast. The Data-Smart City Pod 5/15/2023. Ep57 From Intent to Impact: Mayor Victoria Woodards on Equity. Bloomberg Center for Cities, Harvard University. https://datasmart.hks.harvard.edu/intent-impact-mayor-victoria-woodards-equity [2] Mayors for a Guaranteed Income (June 29, 2020). Press release: Mayors across the U.S. launch gauranteed income initiative. Accessed 6/4/24, https://economicsecurityproject.org/news/mayors-across-the-u-s-launch-guaranteed-income-initiative/ [3] KIRO 7 news. October 5, 2022. Violent crime nearly doubled in the past year. https://www.kiro7.com/news/local/tacoma-mayor-discusses-priorities-city-faces-rising-crime/BTQUAIW5WNEZLE4MSJVZP2KIQI/ [4] United Way of Pierce County. Growing Resilience in Tacoma (GRIT)—a guaranteed income demonstration. Accessed 6/4/24. https://www.uwpc.org/growing-resilience-tacoma-grit-guaranteed-income-demonstration [5] KUOW/ NPR network (8/12/21), Mayor Woodard on how Tacoma’s guaranteed income pilot gives new meaning to ‘grit.’ https://www.kuow.org/stories/tacoma-joins-nationwide-guaranteed-income-pilot-project-ef0d [6] Mayors for a Guaranteed Income home page, accessed 6/4/24. https://www.mayorsforagi.org/ [7] Pega, Frank; Pabayo, Roman; Benny, Claire; Lee, Eun-Young; Lhachimi, Stefan; Liu, Sze (2022). “Unconditional cash transfers for reducing poverty and vulnerabilities: Effect on use of health services and health outcomes in low- and middle-income countries, Cochrane Database of Systematic Reviews. 2022 (3): CD011135. doi:10.1002/14651858.CD011135.pub3. [8] Strozewski, Zoe {7/3/2021), More U.S. mayors interested in gauranteed income programs after early successes, Newsweek. https://www.newsweek.com/more-us-mayors-interested-guaranteed-income-programs-after-early-successes-1612568 Like Trauma Dispatch? You can subscribe to our email notices of new posts on this page. CATEGORY: GOVERNMENT PROJECTS  Left: Nadine Burke Harris, MD, former California Surgeon General. Right: Diana Ramos, M.D., current California Surgeon General Source: Office of California Surgeon General press release Read time: 2.5 minutes This Happened On May 1, 2024, the Office of the California Surgeon General announced the launch of the Live Beyond campaign to increase awareness and understanding of Adverse Childhood Experiences (ACEs) and toxic stress. Who Did This? The Office of the California Surgeon General runs the state’s program to improve the health of citizens by warning them of the presumed dangers of ACEs. The ACE program was started under the inaugural Surgeon General, Nadine Burke Harris, M.D. who served 2019-2022. She is a pediatrician and has a master of public health degree. Harris stepped down in 2022 but continues her advocacy for ACEs independently. Diana Ramos, M.D. has been Surgeon General since 2022. She is an obstetrician, has a master of public health degree, and advocates for equity. The Premise The study that started the ACE movement was published in 1998. This study retrospectively reviewed patient charts and found a correlation between the number of ACEs and physical diseases including heart disease, cancer, lung disease, and obesity [1]. The advocates of ACE made a leap in interpretation to claim that ACEs cause these diseases rather than just being associated for other reasons. Dozens of similar studies have since been conducted that keeps increasing the number of linked physical disease outcomes. As the graphic below shows, the California program makes the claim that the effects of ACEs make individuals more likely to develop 9 of the 10 leading causes of death [2].  The 10 ACEs are: Emotional, verbal abuse Physical abuse Sexual abuse Emotional neglect Physical neglect Divorce / abandoned by parent Domestic violence Parental substance abuse Parental mental illness Family member went to prison California initiated the program in 2020 with the ACEs Aware initiative, a first-in-the-nation attempt to pay primary care providers to screen for the 10 ACE events in children and adults. At the time, Nadine Burke Harris set a goal to reduce ACEs and toxic stress by half in one generation [3]. Their February 2024 update boasted that over 1.5 million individuals had been screened for ACEs from January 1, 2020 to October 31, 2023. The report also asserted that the program made a difference in clinical care but did not report any details [4]. The next phase of the program is the $24 million Live Beyond initiative, which is principally a public relations campaign aimed at 16-25 year-olds. By providing an informational website, social content on Instagram, Facebook, and TikTok, and inspirational stories of healing, the Live Beyond campaign hopes to prevent future ACEs. Analysis The California ACE campaign is based on the premise that you can prevent stress life events by handing out a screen at a doctor visit. One of the co-authors of the 1998 study, Robert Anda, and others, however, voiced their opposition and warned against screening [5]. It is implausible to believe that giving a screen, which may or may not be followed by brief counsel from a doctor about community resources, can prevent ACEs. If it were that simple, complex societal problems would have been shrunk a long time ago. The underlying premise of ACEs is flawed because the studies are flawed. They are cross-sectional and have zero ability to explain causal relationships. Rather than ACEs causing physical diseases, it is more plausible that family settings where ACEs are more likely to happen are the same family settings where worse physical health outcomes are likely to happen. Neither one causes the other. They co-occur in families because bad things in life do not usually happen at random due to complex genetic and heritable reasons. ACE advocates claim that their science cannot be challenged because it is based on a scientific consensus. The problem with that claim is that the field of scholars in academia has become over the past sixty years a self-selected group who are highly skewed toward progressive leftist ideology [6]. The skew is probably even more prominent in leaders of national organizations that produce the consensus statements. Why Is This Happening? The likely true purpose of the campaign is to maintain and tighten control of a public narrative supporting the ideology that humans are highly malleable and children are highly fragile. Hence, rather than promoting nuclear families and self-reliance, the ACE narrative is important for supporting progressive leftist government entitlement programs—under the guise of public health— to supposedly make the world a better place. REFERENCES [1] Vincent J. Felitti et al. "Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. The Adverse Childhood Experiences (ACE) Study," American Journal of Preventive Medicine 14 (1998): 245-258. [2] Live Beyond website. Accessed May 30, 2024. https://livebeyondca.org/parents-caregivers/ [3] Press release, December 9, 2020. Office of the California Surgeon General. https://osg.ca.gov/wp-content/uploads/sites/266/2020/12/PRESS-RELEASE_SG-REPORT_ACES_TOXIC-STRESS_12092020.pdf [4] Quarterly Progress Update, February 2024. Office of the California Surgeon General. https://www.acesaware.org/wp-content/uploads/2024/01/ADA_Feb_2024_Quarterly_Progress_Report_01172024.pdf [5] Robert F. Anda, Laura E. Porter, David W. Brown Inside the Adverse Childhood Experience Score: Strengths, Limitations, and Misapplications. American Journal of Preventive Medicine 2020;59(2):293−295; https://doi.org/10.1016/j.amepre.2020.01.009 John D. McLennan, Andrea Gonzalez, Harriet L. MacMillan, Tracie O. Afifi, Routine screening for adverse childhood experiences (ACEs) still doesn't make sense, Child Abuse & Neglect, 2024, https://doi.org/10.1016/j.chiabu.2024.106708 [6] Mitchell Langbert (2018). Homogenous: The Political Affiliations of Elite Liberal Arts College Faculty. Academic Questions 31:186-197. doi 10.1007/s12129-018-9700-x Like Trauma Dispatch? You can subscribe to our email notices of new posts on this page. CATEGORY: GOVERNMENT PROJECTS: COUNTY  Zoe Lyons, Michigan Department of Health and Human Services, Jackson County Director Source: Washtenaw County government Read time: 3.4 minutes This Happened On April 9, 2024, Washtenaw County government posted on their website about how their Handle With Care Program is successful. Who Is Doing This? Washtenaw County, MI, and the Michigan Department of Health and Human Services The Premise The Handle With Care program appears at first glance to be a simple and innocent-looking intervention. According to the Michigan Implementation Guide: "The Handle With Care Model: If a law enforcement officer encounters a child during a call, that child’s name and three words, HANDLE WITH CARE, are forwarded to the school before the school bell rings the next day. The school implements individual, class and whole school trauma-sensitive strategies so that traumatized children are “Handled With Care.” If a child needs more intervention, on-site trauma-focused mental healthcare is available at the school."[1] The types of situations officers are instructed to report include life-threatening traumas and everyday stressors of neglect, betrayal of trust, the normal loss of a loved one, illness in a caregiver, bullying, and witnessing police activity. The program was first piloted in West Virginia in 2013. Headquartered at the West Virginia Center for Children’s Justice, the program spread to other states. In 2017, the program was launched in Michigan by Zoe Lyons of the Michigan Department of Health and Human Services in Jackson County. The program next spread to Eaton and Washtenaw counties in 2018, and now, according to Second Wave Michigan [2], it is in 49 of 83 Michigan counties. The post noted that since February 2018, when the program was launched, Washtenaw County schools–public and private–have received 3,796 Handle With Care notices from law enforcement officers. The post did not include the number of children in the notices or the base rate of the number of total students in the county. Each notice can include multiple children. Based on a different source [2}, each notice averages 1.5 children, meaning that the 3,796 notices probably involved over 5,700 children. This averages to over 1,100 children annually. The Washtenaw Intermediate School District (WISD) website lists a base rate of 43,482 total students in approximately 130 schools. Hence, notices are received on about 2.5% of students annually. How do schools handle these children differently? First, teachers are instructed to observe for signs of distress, such as inattention, crying, anger, or withdrawal. Then, teachers may reteach a lesson, postpone a test, or suggest the student can go to the nurse’s station to take a nap. If distress is more severe, teachers can call in the school counselor who may meet with the student and may or may not decide to contact parents in order to initiate a referral to outside counseling. The only type of evidence of success in the post was an anecdote when “a substitute teacher looked up to see a student in her class crying. Because she’d seen the notice, she knew to check in with the girl right away, and to refer her to the school social worker for follow-up care.” Analysis “Wanting to help is not the same as helping.” Abigail Shrier, Bad Therapy (2024) This program raises at least five concerns. (1) It is probably not harmless. The program is an intervention for individuals and families who are not seeking one. The field of psychology has been down this road before with research on critical incident stress debriefing which showed repeatedly that making people talk immediately following stressful events often made them worse. The Handle With Care program advises teachers to not ask children to talk about their events, but if they proceed to the higher step of sending them to school counselors, that seems inevitably what will happen. (2) It is a breach of confidentiality. This program flies past the safeguards that other professions, such as health care systems, work under. Federal laws protect the privacy of patients. Doctors face sanctions for disclosing details about patient visits and even for acknowledging that patients attended their clinics. The privacy laws serve to prevent health care professionals from disclosing sensitive information about individuals that could harm the reputations of patients or influence the services they receive (or do not receive). There are few extreme situations where doctors are allowed to violate that privacy. (3) Parents are left out of the loop. The school does not call the student’s home when notices are received or acted upon. It’s a concern that some teachers may use this sensitive information to gain confidence with children or drive wedges between their parents. With the recent revelations that a subset of teachers and schools have implemented critical race theory teaching open racism towards whites, and fostered gender transition activities hidden from parents, it’s not so clear any more how some teachers perceive their role in society. (4) Teachers don’t need notices to pay attention to their students. Teachers already observe their students and make accommodations as needed every day. Also, there are already federal laws for public schools to create accommodations for children with emotional and behavioral problems. The program seems to assert, without data, that teachers don’t already notice changes in their students or make accommodations. It’s not clear that this program provides skills to teachers that they don’t already have. (5) The program is impossible to evaluate. There are no data on what teachers actually do with notices or whether the things they do make any difference for children. It is conceivable that 99% of the notices are unnecessary because children are not distressed, and/or teachers ignore the notices. There is no way to measure whether the effort and taxpayer money invested in the programs make a substantial difference. The only testimony that the program helps is anecdotes. The old maxim, however, “anecdotes are not evidence” is fitting. Why Is This Happening? The program teaches the unproven doctrines of adverse childhood experiences (ACE) and toxic stress that stress and trauma permanently damage brains and physical health. If this is believed, then interventions must be implemented to prevent and alleviate stress on a massive public health scale. This program creates another entry point to indoctrinate professionals in the ACEs and toxic stress narratives. Like Trauma Dispatch? You can subscribe to our email notices of new posts on this page. REFERENCES [1] Michigan Department of Health and Human Services (2019), Handle With Care Michigan Implementation Guide. https://www.michigan.gov/-/media/Project/Websites/mdhhs/Folder4/Folder12/Folder3/Folder112/Folder2/Folder212/Folder1/Folder312/Handle_With_Care_Implementation_Guide_Final.pdf?rev=f6d24de6ca41417494783ffb6f37518e. Accessed 5/7/2024. [2] Slootmaker E (December 8, 2022), State program helps Michigan schools handle students with extra care if they've experienced trauma, Second Wave Michigan. https://www.secondwavemedia.com/features/handlewithcare12082022.aspx. Accessed 5/7/24. Can you model social change as linear line graphs? The Cincinnati City Council presentation5/4/2024
CATEGORY: GOVERNMENT PROJECTS: CITY  Daniel Chen, DrPH, George Washington University Source: Cincinnati City Council Read time: 2.4 minutes plus a short video This Happened A professor of public health demonstrated a “system dynamics modeling” software program as one component of a larger plan to persuade Cincinnati city government to implement systemic social changes. The professor was one of six presenters in the group who came before a committee of the Cincinnati City Council on April 2, 2024. Who Did This? Daniel Chen, DrPH, from the Global Health Department of George Washington University’s school of public health, presented the software. He has been the first author on one peer-reviewed paper and secondary author on five others focused mostly on trauma-informed care. The Presentation Chen’s software demonstration was one component of a larger strategy claiming that adverse childhood experiences (ACE) cause permanent brain and body damage that leads to a wide variety of mental problems, physical diseases, and social dysfunctions. Hence, the group argued, government investments are needed to relieve these stressors. The purpose of the software modeling is to provide a tool for policy makers to make informed decisions. Chen said his system dynamics modeling was based on 300 variables and about 500 equations. For the first simulation, Chen input a “policy lever” on the model’s dashboard—a program to provide financial assistance for renters to become homeowners. The model then spit out a line graph to show how the percentage of homeowners increased every year. A bit later, Chen input another policy lever to provide financial assistance to prevent foreclosures, and again, this produced a line graph, this time showing, predictably, fewer foreclosures every year. Lastly, Chen ran both policy levers simultaneously to show how they would impact “population health” by increasing the number of individuals with Good or Excellent Health. Analysis One concern about modeling of complex public health problems, in general, has been unreliability. Take, for instance, the infamous Imperial College London model at the beginning of the COVID-19 pandemic that predicted peak mortalities above 215 deaths per million in Great Britain. This announcement played a large role world-wide to drive harsh distancing measures and lockdowns. In reality, Great Britain flattened the curve at 13.9 deaths per million [1]. The COVID model failed because the humans using it made pessimistic and unchanging guesses about the infection rate, death rate, time to recovery, and the rate of passing the virus between persons. In addition, it did not account for motivations to misattribute deaths to COVID, how lockdowns would prolong the epidemic, or how therapeutics would shorten it. Put simply, almost nothing in nature or human society changes in a straight line. The video (below) shows the first simulation. As noted above, Chen inputs a “policy lever” on the model’s dashboard—a program, called ADDI, to provide financial assistance for renters to become homeowners. He set the lever at 1% in the neighborhood of Avondale starting in 2025, meaning that of 4,085 renters, 40 would become homeowners the next year, and 1% more would be added in each successive year. The percentage of homeowners increased from about 25% in 2025 to a nearly miraculous 50% in 2055. As you watch the line graph in the upper right, note how it is a perfectly straight upward-trending line for thirty years. Another concern, and perhaps the inherent fatal flaw of models, is that they almost never can predict how individual behaviors vary over time. Consider Daniel Partick Moynihan’s famous scissors graph in his 1965 report (below). For decades, as unemployment for nonwhite males rose or fell, applications for welfare logically rose or fell in tandem. But in 1960, something changed; unemployment dropped but applications for welfare increased. Moynihan attributed this to a shift in Black family structure towards single-parent households. Put simply, almost nothing changes in the real world as policy makers intend. 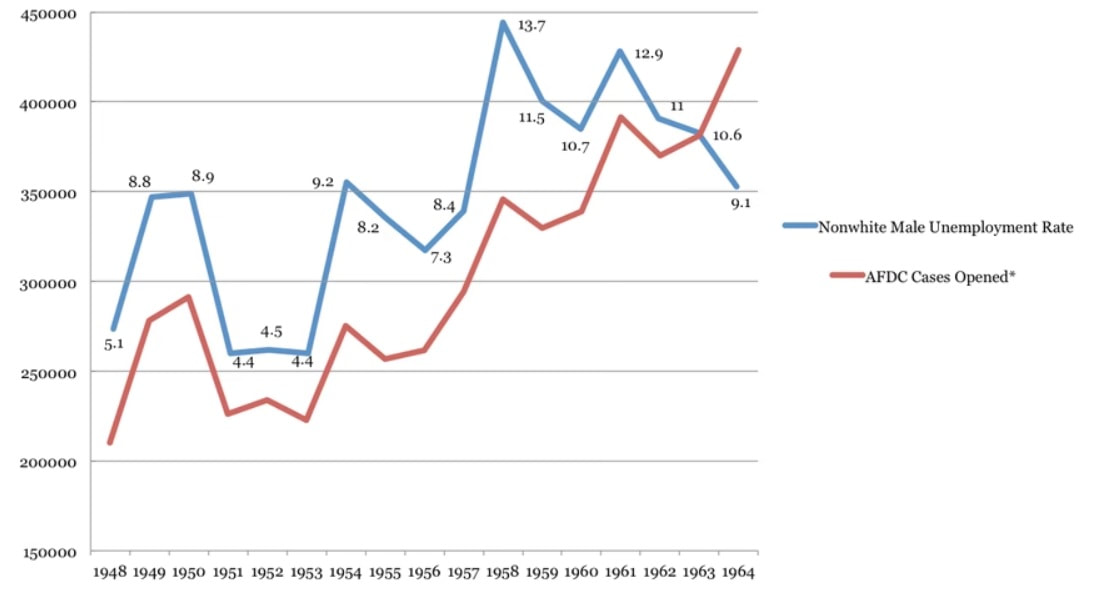 In the graph above, note how, starting in 1960, unemployment and applications for Aid to Families With Dependent Children (AFDC) welfare assistance suddenly went in opposite directions [2]. When showing models in this manner to legislators, it can easily be misleading:
Chen and his group pitched the model as being based on empirical evidence, when actually it’s based on a utopian idea that everything goes according to their plan. Like Trauma Dispatch? You can subscribe to our email notices of new posts on this page. References [1] Boretti A. After Less Than 2 Months, the Simulations That Drove the World to Strict Lockdown Appear to be Wrong, the Same of the Policies They Generated. Health Serv Res Manag Epidemiol. 2020 Jun 17;7:2333392820932324. doi: 10.1177/2333392820932324. PMID: 32596417; PMCID: PMC7301657. [2] Daniel Geary, The Moynihan Report: An annotated edition, The Atlantic, September 14, 2015. Accessed May 4, 2024. CATEGORY: GOVERNMENT PROJECTS: STATE  Bill sponsors, clockwise from top left: Dafna Michaelson Jenet (D), Brianna Titone (D), Nancy Todd (D), and Dennis Hisey (R) Source: 9News Denver and Colorado H.B.20-1312 Read time: 2.7 minutes plus video This Happened Denver’s 9News outlet ran a story April 4, 2024 on the implementation of Colorado’s new mandate for training of teachers in trauma-informed practices (TIP). The law was passed and took effect in 2020. Who Did This? Sponsors of the bill were Rep. Dafna Michaelson Jenet (D) (now a state senator), Rep. Brianna Titone (D), Sen. Dennis Hisey (R) (served one term before losing reelection in 2022), and Sen. Nancy Todd (D) (left office in 2021 after a sixteen-year career). Titone, born a biological male, was the first openly transgender person elected to the Colorado legislature. The Premise The theory of TIP is that trauma-exposed individuals ought to be sensitively handled by professionals in many spheres to both prevent worsening through re-traumatization and promote healing through new knowledge and skills. The mandate comes from Colorado Statute § 22-60.5-110, Section 3.f., which dictates conditions for renewal of professional teacher licenses. It includes the following:
The text of the bill did not provide a rationale as to why this type of training would facilitate teachers’ skills and competence in the delivery of academic instruction. While the law covers teachers in all grades, the 9News story focused on the launch of the mandate within Colorado’s universal pre-K program. Anchor Corey Rose chatted with Dr. Rosemarie Allen, the station’s “race and equity expert.” Allen’s doctorate is in Equity and Leadership in Education; she is the president and CEO for the nonprofit Institute for Racial Equity and Excellence which licenses child care providers in Colorado. In the 1.3-minute video below, Dr. Allen asserted that trauma impacts child development, and this new training will give teachers “amazing strategies.” Analysis The premise of TIP is based on several controversial assertions. (1) It is based on the ideology that trauma permanently damages the brain and derails child development, neither of which are proven. (2) The concept of TIP is not a clear or testable theory. TIP can be any or all of the following: train professionals, professional self-care, educate victims, teach coping skills, tweak customer service to avoid retraumatizing victims, arrange environments to make people feel safer, include trauma victims in advisory roles, track customer satisfaction outcomes, communicate between service areas, allow drop-in service, change hiring practices, create women-only environments, and, of course, direct clinical care to treat trauma symptoms. Many of these do not represent evident mechanisms or effective paths to improve victim outcomes. (3) Besides direct clinical care, the interventions by themselves or in combination have not been shown to consistently improve mental health or learning outcomes. Nearly all the non-clinical studies on TIP have measured perceptions of professionals on whether they believe they and/or their workplace are better informed or more competent. (4) In regards to school settings, it is controversial whether teachers ought to be assuming responsibilities that have previously belonged only to parents to intervene in social and emotional issues outside their scope of expertise. The Colorado legislature estimated the cost of this program to the state to be between $8,000 to $600,000. Why Is This Happening? Despite assertions by supporters, TIP is not an empirically-driven scientific model. It is an ideological-based movement consistent with progressive leftist ideas that humans are highly malleable. Statutes like this have been adopted in a growing number of states and cities to authorize government interventions in a wide range of environments. Direct clinical trauma care, based on evidence, and delivered with common sense of sensitive and empathic professionals, has been commonly available for over three decades. What’s new in TIP is the mandate to train non-clinical professionals and trauma victims on an ideology, embed this model into statute, and create new administrative agencies and infrastructures that will inevitably increase in size and cost over time. Like Trauma Dispatch? You can subscribe to our email notices of new posts on this page. CATEGORY: GOVERNMENT PROJECTS: CITY  Wendy Ellis, Dr.P.H., Assistant Professor, George Washington University Source: WCPO ABC 9 news Read time: 1.7 minutes This Happened On April 2, 2024, a committee of the Cincinnati City Council hosted a presentation titled Building Equitable & Resilient Neighborhoods. This was the latest step in a process over recent years by a coalition of community leaders demanding government action for large-scale systemic change by trying to address stress and trauma as underlying causes of inequity in child outcomes. Who Did This? The coalition consists of Cincinnati Children’s Hospital, the University of Cincinnati, and George Washington University’s Center for Community Resilience. The group presentation was led by Wendy Ellis, Assistant Professor at George Washington University. Her 2019 dissertation was a model that conceptualizes adverse childhood experiences (ACEs) as outcomes of systems driven by institutional racism; and these outcomes, including racial disparities in evictions, income inequity, and economic mobility, must be addressed through public health initiatives. The Premise The coalition is trying to press city government to adopt new policies and enact reforms aimed at addressing trauma because they assert those cause inequities in child well-being outcomes. Their language tends to emphasize trauma, but their model includes everyday stress experiences—household disruption, parental incarceration, food insecurity, and poverty—that are not life-threatening trauma. Proposed reforms include to alleviate poverty (cash assistance, child tax credits), increase entitlements (preschool and childcare), educate children on relationship skills, educate parents on how to parent, provide mentoring and after-school programs, and teach everyone about the ACEs narrative.
Analysis Consistent with the postmodern trauma activism of the past several decades that draws extraordinary causal interpretations from shaky science, these ACEs models claim to understand for the first time in history what drives nearly all human suffering. It cannot be overemphasized that supporters of ACE movements intend large-scale expansion of entitlements and government power. Their intent is to “transform,” as the subtitle of the presentation stated: “Vision: Transform the City of Cincinnati into a national beacon of healing, community resilience, and racial justice by centering the experiences and interests of trauma exposed children and families in organizational planning, partnerships, and policies.” Philadelphia, Baltimore, New Orleans, and other cities have embarked on similar public health models based on the ACEs narrative. Each are different in details and stage of implementation, but none have achieved major success. No reports from these models have provided evidence that these strategies work. It is unlikely the programs can work because the ACE research on which they are built is controversial and unproven. Dr. Ellis says “The science is clear,” but she and other ACE supporters seem unaware that all ACE research comes from cross-sectional studies that have zero power to prove causative links. Another concern, besides the science, is that none of this reform for large-scale culture shift has been adequately presented to or voted on by the public, who are mostly unaware of what is happening. Like Trauma Dispatch? You can subscribe to our email notices of new posts on this page. |
